
Cubital Tunnel: The “Other” Tunnel
2 Comments“Just one more page.” One minute you’re being pulled into a great mystery novel and the next thing…your fingers are tingling. Shaking out your hand and moving your elbow in and out seem to return your fingers to normal but a few pages later, the tingling returns, especially in the small finger. Perhaps your first thought is, “Carpal tunnel syndrome.” A quick Internet search only causes more confusion. You might have cubital tunnel syndrome.
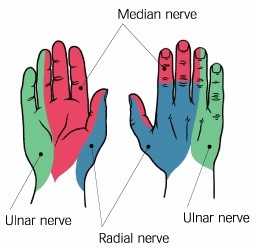
Cubital tunnel syndrome (CTS), despite being the second most common nerve compression syndrome in the arm1, is less known to lay population than carpal tunnel syndrome. Similar to carpal tunnel syndrome the name refers to compression of the nerve where the nerve has to pass through a narrow area, i.e., the tunnel. However, CTS does differ from carpal tunnel syndrome in several key areas. The site of compression is located at the elbow compared to the wrist for carpal tunnel syndrome. The nerve affected is the ulnar nerve, which provides sensation to all sides of the small finger as well as to the small finger side of the ring finger. Conversely, carpal tunnel syndrome involves a branch of the median nerve and provides sensation to the a portion of the thumb, index, and middle fingers and the remaining portion of the ring finger on the palm side and the tips on the back side. (See schematic.) There is a previous blog post about carpal tunnel syndrome here (hyperlink) that can explain it in greater detail.
 Although there are minor variances, in CTS the area of compression is located at the medial (inside) portion of the elbow, and this compression is enhanced when the elbow is bent, such as with reading. Other positions that may increase symptoms are talking on the phone, driving, and sleeping. The easiest self-treatment for cubital tunnel syndrome is avoiding these positions, which all require sustained elbow flexion. Taking frequent breaks while reading and talking on the phone to straighten elbow as well as keeping elbow in a slightly flexed (as opposed to fully flexed) position while sleeping can help alleviate symptoms. A skilled hand therapist can fabricate an orthosis to help maintain the elbow in this position at nighttime as well as instruct on ways to help the nerve glide through the length of the arm and how to maintain general upper extremity flexibility.
Although there are minor variances, in CTS the area of compression is located at the medial (inside) portion of the elbow, and this compression is enhanced when the elbow is bent, such as with reading. Other positions that may increase symptoms are talking on the phone, driving, and sleeping. The easiest self-treatment for cubital tunnel syndrome is avoiding these positions, which all require sustained elbow flexion. Taking frequent breaks while reading and talking on the phone to straighten elbow as well as keeping elbow in a slightly flexed (as opposed to fully flexed) position while sleeping can help alleviate symptoms. A skilled hand therapist can fabricate an orthosis to help maintain the elbow in this position at nighttime as well as instruct on ways to help the nerve glide through the length of the arm and how to maintain general upper extremity flexibility.
Individuals with diabetes mellitus are more susceptible to CTS, as they are with other nerve compression syndromes. Obesity is also correlated with those prone to this syndrome. There is some evidence that job demands can increase incidence of CTS, such as repetitive tool usage and vibration.1
It is important to address symptoms early with both activity modification and flexibility exercises as prolonged compression on a nerve is difficult to reverse conservatively (without surgery) and can cause loss of strength in muscles that rely on the ulnar nerve for innervation. For the ulnar nerve these muscles are dispersed throughout the hand and are beyond the scope of this blog but can affect ability to produce a strong grip as well as to pinch with the thumb.
So next time you find yourself deeply engrossed in a great mystery and you’re noticing ‘mysterious’ tingling in your small finger, don’t ignore these syndromes. Take a break to adjust your elbow position, and if you find your symptoms are affecting you daily, don’t hesitate to follow up with a complimentary injury screen from Athletico’s hand specialists.
- Cutts, S (2007). Cubital Tunnel Syndrome. Postgrad Medical Journal. Vol. 83(975): 28-31


2 Comments
Rose McAndrew
Thanks for the comment, Dr. Martino. I’m not familiar with the Lonnie Brace, so I will take a look at your link. Any suggestions for this often challenging diagnosis are appreciated.
Mary Ann Baxter
Thank you so much for this detailed information on Cubital Tunnel Syndrome. My little finger and ring finger on my right hand have been numb, forearm very painful and grip strength down to nil, over the past 3 years. I had PT for tennis elbow, but pain still goes on, although my grip strength has improved. My PT told me my ulnar nerve was the problem but it didn’t go much further for treatment. I will be wrapping a towel around my arm at night to keep it straight from now on, thank to your very informative site. Thanks!